From Wikipedia, the free encyclopedia
Not to be confused with Narcosis.

Structural changes of cells undergoing necrosis and apoptosis
Necrosis (from Ancient Greek νέκρωσις (nékrōsis) ‘death’) is a form of cell injury which results in the premature death of cells in living tissue by autolysis.[1] Necrosis is caused by factors external to the cell or tissue, such as infection, or trauma which result in the unregulated digestion of cell components. In contrast, apoptosis is a naturally occurring programmed and targeted cause of cellular death. While apoptosis often provides beneficial effects to the organism, necrosis is almost always detrimental and can be fatal.[2]
Cellular death due to necrosis does not follow the apoptotic signal transduction pathway, but rather various receptors are activated and result in the loss of cell membrane integrity[3] and an uncontrolled release of products of cell death into the extracellular space.[1] This initiates in the surrounding tissue an inflammatory response, which attracts leukocytes and nearby phagocytes which eliminate the dead cells by phagocytosis. However, microbial damaging substances released by leukocytes would create collateral damage to surrounding tissues.[4] This excess collateral damage inhibits the healing process. Thus, untreated necrosis results in a build-up of decomposing dead tissue and cell debris at or near the site of the cell death. A classic example is gangrene. For this reason, it is often necessary to remove necrotic tissue surgically, a procedure known as debridement.[citation needed]
Classification[edit]
Structural signs that indicate irreversible cell injury and the progression of necrosis include dense clumping and progressive disruption of genetic material, and disruption to membranes of cells and organelles.[5]
Morphological patterns[edit]
There are six distinctive morphological patterns of necrosis:[6]
- Coagulative necrosis is characterized by the formation of a gelatinous (gel-like) substance in dead tissues in which the architecture of the tissue is maintained,[6] and can be observed by light microscopy. Coagulation occurs as a result of protein denaturation, causing albumin to transform into a firm and opaque state.[5] This pattern of necrosis is typically seen in hypoxic (low-oxygen) environments, such as infarction. Coagulative necrosis occurs primarily in tissues such as the kidney, heart and adrenal glands.[5] Severe ischemia most commonly causes necrosis of this form.[7]
- Liquefactive necrosis (or colliquative necrosis), in contrast to coagulative necrosis, is characterized by the digestion of dead cells to form a viscous liquid mass.[6] This is typical of bacterial, or sometimes fungal, infections because of their ability to stimulate an inflammatory response. The necrotic liquid mass is frequently creamy yellow due to the presence of dead leukocytes and is commonly known as pus.[6] Hypoxic infarcts in the brain presents as this type of necrosis, because the brain contains little connective tissue but high amounts of digestive enzymes and lipids, and cells therefore can be readily digested by their own enzymes.[5]
- Gangrenous necrosis can be considered a type of coagulative necrosis that resembles mummified tissue. It is characteristic of ischemia of lower limb and the gastrointestinal tracts. If superimposed infection of dead tissues occurs, then liquefactive necrosis ensues (wet gangrene).[8]
- Caseous necrosis can be considered a combination of coagulative and liquefactive necrosis,[5] typically caused by mycobacteria (e.g. tuberculosis), fungi and some foreign substances. The necrotic tissue appears as white and friable, like clumped cheese. Dead cells disintegrate but are not completely digested, leaving granular particles.[5] Microscopic examination shows amorphous granular debris enclosed within a distinctive inflammatory border.[6] Some granulomas contain this pattern of necrosis.[9]
- Fat necrosis is specialized necrosis of fat tissue,[9] resulting from the action of activated lipases on fatty tissues such as the pancreas. In the pancreas it leads to acute pancreatitis, a condition where the pancreatic enzymes leak out into the peritoneal cavity, and liquefy the membrane by splitting the triglyceride esters into fatty acids through fat saponification.[6] Calcium, magnesium or sodium may bind to these lesions to produce a chalky-white substance.[5] The calcium deposits are microscopically distinctive and may be large enough to be visible on radiographic examinations.[7] To the naked eye, calcium deposits appear as gritty white flecks.[7]
- Fibrinoid necrosis is a special form of necrosis usually caused by immune-mediated vascular damage. It is marked by complexes of antigen and antibodies, referred to as immune complexes deposited within arterial walls[6] together with fibrin.[6]
Other clinical classifications of necrosis[edit]
- There are also very specific forms of necrosis such as gangrene (term used in clinical practices for limbs which have had severe hypoxia), gummatous necrosis (due to spirochaetal infections) and hemorrhagic necrosis (due to the blockage of venous drainage of an organ or tissue).
- Some spider bites may lead to necrosis. In the United States, only spider bites from the brown recluse spider (genus Loxosceles) reliably progress to necrosis. In other countries, spiders of the same genus, such as the Chilean recluse in South America, are also known to cause necrosis. Claims that yellow sac spiders and hobo spiders possess necrotic venom have not been substantiated.
- In blind mole rats (genus Spalax), the process of necrosis replaces the role of the systematic apoptosis normally used in many organisms. Low oxygen conditions, such as those common in blind mole rats’ burrows, usually cause cells to undergo apoptosis. In adaptation to higher tendency of cell death, blind mole rats evolved a mutation in the tumor suppressor protein p53 (which is also used in humans) to prevent cells from undergoing apoptosis. Human cancer patients have similar mutations, and blind mole rats were thought to be more susceptible to cancer because their cells cannot undergo apoptosis. However, after a specific amount of time (within 3 days according to a study conducted at the University of Rochester), the cells in blind mole rats release interferon-beta (which the immune system normally uses to counter viruses) in response to over-proliferation of cells caused by the suppression of apoptosis. In this case, the interferon-beta triggers cells to undergo necrosis, and this mechanism also kills cancer cells in blind mole rats. Because of tumor suppression mechanisms such as this, blind mole rats and other spalacids are resistant to cancer.[10][11]
Causes[edit]

Necrosis may occur due to external or internal factors.
External factors[edit]
External factors may involve mechanical trauma (physical damage to the body which causes cellular breakdown), damage to blood vessels (which may disrupt blood supply to associated tissue), and ischemia.[12] Thermal effects (extremely high or low temperature) can result in necrosis due to the disruption of cells.[citation needed]
In frostbite, crystals form, increasing the pressure of remaining tissue and fluid causing the cells to burst.[citation needed] Under extreme conditions tissues and cells die through an unregulated process of destruction of membranes and cytosol.[13]
Internal factors[edit]
Internal factors causing necrosis include: trophoneurotic disorders (diseases that occur due to defective nerve action in a part of an organ which results in failure of nutrition); injury and paralysis of nerve cells. Pancreatic enzymes (lipases) are the major cause of fat necrosis.[12]
Necrosis can be activated by components of the immune system, such as the complement system; bacterial toxins; activated natural killer cells; and peritoneal macrophages.[1] Pathogen-induced necrosis programs in cells with immunological barriers (intestinal mucosa) may alleviate invasion of pathogens through surfaces affected by inflammation.[1] Toxins and pathogens may cause necrosis; toxins such as snake venoms may inhibit enzymes and cause cell death.[12] Necrotic wounds have also resulted from the stings of Vespa mandarinia.[14]
Pathological conditions are characterized by inadequate secretion of cytokines. Nitric oxide (NO) and reactive oxygen species (ROS) are also accompanied by intense necrotic death of cells.[12] A classic example of a necrotic condition is ischemia which leads to a drastic depletion of oxygen, glucose, and other trophic factors and induces massive necrotic death of endothelial cells and non-proliferating cells of surrounding tissues (neurons, cardiomyocytes, renal cells, etc.).[1] Recent cytological data indicates that necrotic death occurs not only during pathological events but it is also a component of some physiological process.[12]
Activation-induced death of primary T lymphocytes and other important constituents of the immune response are caspase-independent and necrotic by morphology; hence, current researchers have demonstrated that necrotic cell death can occur not only during pathological processes, but also during normal processes such as tissue renewal, embryogenesis, and immune response.[12]
Pathogenesis[edit]
Pathways[edit]
Until recently, necrosis was thought to be an unregulated process.[15] However, there are two broad pathways in which necrosis may occur in an organism.[15]
The first of these two pathways initially involves oncosis, where swelling of the cells occurs.[15] Affected cells then proceed to blebbing, and this is followed by pyknosis, in which nuclear shrinkage transpires.[15] In the final step of this pathway cell nuclei are dissolved into the cytoplasm, which is referred to as karyolysis.[15]
The second pathway is a secondary form of necrosis that is shown to occur after apoptosis and budding.[15] In these cellular changes of necrosis, the nucleus breaks into fragments (known as karyorrhexis).[15]
Histopathological changes[edit]
The nucleus changes in necrosis and characteristics of this change are determined by the manner in which its DNA breaks down:
- Karyolysis: the chromatin of the nucleus fades due to the loss of the DNA by degradation.[6]
- Karyorrhexis: the shrunken nucleus fragments to complete dispersal.[6]
- Pyknosis: the nucleus shrinks, and the chromatin condenses.[6]
Other typical cellular changes in necrosis include:
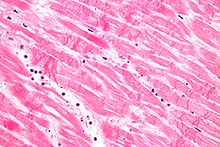
- Cytoplasmic hypereosinophilia on samples with H&E stain.[16] It is seen as a darker stain of the cytoplasm.
- The cell membrane appears discontinuous when viewed with an electron microscope. This discontinuous membrane is caused by cell blebbing and the loss of microvilli.[6]
On a larger histologic scale, pseudopalisades (false palisades) are hypercellular zones that typically surround necrotic tissue. Pseudopalisading necrosis indicates an aggressive tumor.[17]
-

Cytoplasmic hypereosinophilia (seen in left half of image)

Treatment[edit]
There are many causes of necrosis, and as such treatment is based upon how the necrosis came about. Treatment of necrosis typically involves two distinct processes: Usually, the underlying cause of the necrosis must be treated before the dead tissue itself can be dealt with.[citation needed]
- Debridement, referring to the removal of dead tissue by surgical or non-surgical means, is the standard therapy for necrosis. Depending on the severity of the necrosis, this may range from removal of small patches of skin to complete amputation of affected limbs or organs. Chemical removal of necrotic tissue is another option in which enzymatic debriding agents, categorised as proteolytic, fibrinolytic or collagenases, are used to target the various components of dead tissue.[18] In select cases, special maggot therapy using Lucilia sericata larvae has been employed to remove necrotic tissue and infection.[19]
- In the case of ischemia, which includes myocardial infarction, the restriction of blood supply to tissues causes hypoxia and the creation of reactive oxygen species (ROS) that react with, and damage proteins and membranes. Antioxidant treatments can be applied to scavenge the ROS.[20]
- Wounds caused by physical agents, including physical trauma and chemical burns, can be treated with antibiotics and anti-inflammatory drugs to prevent bacterial infection and inflammation. Keeping the wound clean from infection also prevents necrosis.
- Chemical and toxic agents (e.g. pharmaceutical drugs, acids, bases) react with the skin leading to skin loss and eventually necrosis. Treatment involves identification and discontinuation of the harmful agent, followed by treatment of the wound, including prevention of infection and possibly the use of immunosuppressive therapies such as anti-inflammatory drugs or immunosuppressants.[21] In the example of a snake bite, the use of anti-venom halts the spread of toxins whilst receiving antibiotics to impede infection.[22]
Even after the initial cause of the necrosis has been halted, the necrotic tissue will remain in the body. The body’s immune response to apoptosis, which involves the automatic breaking down and recycling of cellular material, is not triggered by necrotic cell death due to the apoptotic pathway being disabled.[23]
In plants[edit]
If calcium is deficient, pectin cannot be synthesized, and therefore the cell walls cannot be bonded and thus an impediment of the meristems. This will lead to necrosis of stem and root tips and leaf edges.[24] For example, necrosis of tissue can occur in Arabidopsis thaliana due to plant pathogens.[citation needed]
Cacti such as the Saguaro and Cardon in the Sonoran Desert experience necrotic patch formation regularly; a species of Dipterans called Drosophila mettleri has developed a p450 detoxification system to enable it to use the exudates released in these patches to both nest and feed larvae.[citation needed]
See also[edit]
![]()
Wikimedia Commons has media related to Necrosis.
- Avascular necrosis
- Frostbite
- Gangrene
- Necrotizing fasciitis
- Osteonecrosis of the jaw
- Toxic epidermal necrolysis
- Necroptosis
References[edit]
- ^ a b c d e Proskuryakov SY, Konoplyannikov AG, Gabai VL (2003). «Necrosis: a specific form of programmed cell death?». Exp. Cell Res. 283 (1): 1–16. doi:10.1016/S0014-4827(02)00027-7. PMID 12565815.
- ^ Kasper DL, Zaleznik DF (2001). «Gas gangrene, antibiotic associated colitis, and other Clostridial infections». In Stone RM (ed.). Harrison’s principles of internal medicine self-assessment and board review (15th ed.). New York: McGraw-Hill, Medical Pub. Division. pp. 922–927. ISBN 978-0071386784.
- ^ Nirmala GJ, Lopus M (2020). «Cell death mechanisms in eukaryotes». Cell Biol Toxicol. 36 (2): 145–164. doi:10.1007/s10565-019-09496-2. PMID 31820165. S2CID 208869679.
- ^ Rock, Kenneth (2008). «The inflammatory response to cell death». Annual Review of Pathology. 3: 99–126. doi:10.1146/annurev.pathmechdis.3.121806.151456. PMC 3094097. PMID 18039143.
- ^ a b c d e f g Craft J, Gordon C, Tiziani A, Huether SE, McCance KL, Brashers VL (2010). Understanding pathophysiology (1st ed.). Chatswood, N.S.W.: Elsevier Australia. ISBN 978-0729539517.
- ^ a b c d e f g h i j k l Kumar V, Abbas AK, Aster JC, Fausto N (2010). Robbins and Cotran pathologic basis of disease (8th ed.). Philadelphia, PA: Saunders/Elsevier. pp. 12–41. ISBN 978-1416031215.
- ^ a b c McConnell TH (2007). The nature of disease: pathology for the health professions. Baltimore, Mar.: Lippincott Williams & Wilkins. ISBN 978-0781753173.
- ^ Sattar (2015). Fundamentals of Pathology (2015th ed.). Chicago, IL: Pathoma LLC. p. 5. ISBN 978-0-9832246-2-4.
- ^ a b Stevens A, Lowe JS, Young B, Deakin PJ (2002). Wheater’s basic histopathology: a colour atlas and text (4th ed.). Edinburgh: Churchill Livingstone. ISBN 978-0443070013.
- ^ Saey, Tina Hesman (5 November 2012). «Cancer cells self-destruct in blind mole rats». Science News. Society for Science and the Public. Archived from the original on 19 June 2013. Retrieved 27 November 2012.
- ^ Gorbunova V, Hine C, Tian X, Ablaeva J, Gudkov AV, Nevo E, Seluanov A (2012). «Cancer resistance in the blind mole rat is mediated by concerted necrotic cell death mechanism». Proc. Natl. Acad. Sci. U.S.A. 109 (47): 19392–6. Bibcode:2012PNAS..10919392G. doi:10.1073/pnas.1217211109. PMC 3511137. PMID 23129611.
- ^ a b c d e f Raffray M, Cohen GM; Cohen (1997). «Apoptosis and necrosis in toxicology: a continuum or distinct modes of cell death?». Pharmacol. Ther. 75 (3): 153–77. doi:10.1016/s0163-7258(97)00037-5. PMID 9504137.
- ^ Nazarian RM, Van Cott EM, Zembowicz A, Duncan LM (2009). «Warfarin-induced skin necrosis». J. Am. Acad. Dermatol. 61 (2): 325–32. doi:10.1016/j.jaad.2008.12.039. PMID 19615543.
- ^ Yanagawa, Youichi (10 October 1980). «Cutaneous hemorrhage or necrosis findings after Vespa mandarinia (wasp) stings may predict the occurrence of multiple organ injury: A case report and review of literature». Clinical Toxicology. 45 (7): 803–807. doi:10.1080/15563650701664871. PMID 17952752. S2CID 11337426.
- ^ a b c d e f g Kroemer G, Galluzzi L, Vandenabeele P, Abrams J, Alnemri ES, Baehrecke EH, Blagosklonny MV, El-Deiry WS, Golstein P, Green DR, Hengartner M, Knight RA, Kumar S, Lipton SA, Malorni W, Nuñez G, Peter ME, Tschopp J, Yuan J, Piacentini M, Zhivotovsky B, Melino G, Nomenclature Committee on Cell Death 2009 (January 2009). «Classification of cell death: recommendations of the Nomenclature Committee on Cell Death 2009». Cell Death Differ. 16 (1): 3–11. doi:10.1038/cdd.2008.150. PMC 2744427. PMID 18846107.
- ^ page 320 Archived 2020-08-04 at the Wayback Machine in: Alberto M Marchevsky; Bonnie Balzer; Fadi W Abdul-Karim (2014). Intraoperative Consultation E-Book: A Volume in the Series: Foundations in Diagnostic Pathology. Elsevier Health Sciences. ISBN 978-0-323-32299-7. Archived from the original on 2020-08-07. Retrieved 2020-01-03.
- ^ Wippold FJ, Lämmle M, Anatelli F, Lennerz J, Perry A (2006). «Neuropathology for the neuroradiologist: palisades and pseudopalisades». AJNR Am J Neuroradiol. 27 (10): 2037–41. PMC 7977220. PMID 17110662.
- ^ Singhal A, Reis ED, Kerstein MD (2001). «Options for nonsurgical debridement of necrotic wounds». Adv Skin Wound Care. 14 (2): 96–100, quiz 102–3. doi:10.1097/00129334-200103000-00014. PMID 11899913.
- ^ Horobin AJ, Shakesheff KM, Pritchard DI (2005). «Maggots and wound healing: an investigation of the effects of secretions from Lucilia sericata larvae upon the migration of human dermal fibroblasts over a fibronectin-coated surface». Wound Repair Regen. 13 (4): 422–33. doi:10.1111/j.1067-1927.2005.130410.x. PMID 16008732. S2CID 7861732.
- ^ Eum HA, Cha YN, Lee SM (2007). «Necrosis and apoptosis: sequence of liver damage following reperfusion after 60 min ischemia in rats». Biochem. Biophys. Res. Commun. 358 (2): 500–5. doi:10.1016/j.bbrc.2007.04.153. PMID 17490613.
- ^ Cooper KL (2012). «Drug reaction, skin care, skin loss». Crit Care Nurse. 32 (4): 52–9. doi:10.4037/ccn2012340. PMID 22855079.
- ^ Chotenimitkhun R, Rojnuckarin P; Rojnuckarin (2008). «Systemic antivenom and skin necrosis after green pit viper bites». Clin Toxicol. 46 (2): 122–5. doi:10.1080/15563650701266826. PMID 18259959. S2CID 6827421.
- ^ Edinger AL, Thompson CB; Thompson (2004). «Death by design: apoptosis, necrosis and autophagy». Curr. Opin. Cell Biol. 16 (6): 663–9. doi:10.1016/j.ceb.2004.09.011. PMID 15530778.
- ^ Capon B (2010). Botany for gardeners (3rd ed.). Portland, OR: Timber Press. ISBN 978-1-60469-095-8.
External links[edit]
- Life In The Fast Lane: toxicology Conundrum #018
- Undersea and Hyperbaric Medical Society. «Necrotizing Soft Tissue Infections». Archived from the original on 5 July 2008. Retrieved 25 July 2008.
- Secondary necrosis of a neutrophil
Некроз – это патологический процесс, выражающийся в местной гибели ткани в живом организме в результате какого-либо экзо- или эндогенного её повреждения.Некроз не только патологический процесс, но и необходимый компонент нормальной жизнедеятельности клеток и тканей в процессе физиологической регенерации. Такое патологическое состояние крайне опасно для человека, чревато самыми тяжелыми последствиями и требует лечения под наблюдением специалистов.
Когда протекает некроз, лечение будет успешным, если заболевание обнаружено на ранней стадии.
Хирурги Научно-практического центра хирургии владеют множеством методик консервативного, щадящего и функционального лечения некроза, а благодаря их высокой квалификации, могут с точностью определить какая из них наилучшим образом подойдет для максимально эффективного результата.
Причины некроза
· Огнестрельные ранения
· Радиационное обучение
· Травмы от удара током
· Ожоги
· Обморожения
· Воздействие токсинов и некоторых химических веществ
· Аллергические и аутоиммунные реакции
· Бактерицидные и вирусные инфекции
· Развитие инфарктов различной этиологии
· Незаживающие язвы и пролежни
Симптомы некроза:
· Онемение, отсутствие чувствительности
· Наблюдается сначала бледность кожных покровов, затем цвет становится синим, темно-зеленым или черным
· Снижение иммунитета
· Нарушение кровообращения
· Нарушение дыхательной системы
В зависимости какие изменения происходят в тканях, выделяют две формы некроза:
· Коагуляционный (сухой) некроз – возникает, когда тканевый белок сворачивается, уплотняется, высыхает и преобразуется в творожистую массу.
· Колликвационный (влажный) некроз – проявляется набуханием, размягчением мертвых тканей, образованием массы серого цвета и появлением запаха гнили.
Виды некроза:
· Инфаркт – возникает в результате внезапного прекращения кровоснабжения в очаге ткани или органа
· Секвестр – омертвевший участок костной ткани располагается в секвестральной полости, отделяется от здоровой ткани по причине гнойного процесса
· Гангрена – омертвение кожи, слизистых поверхностей и мышц. Ее развитию предшествует некроз тканей.
· Пролежни – возникают у обездвиженных людей вследствие длительного сдавливания тканей. Это приводит к образованию гнойных язв.
Стадии некротического процесса:
1. Паранекроз – обратимые дистрофические изменения
2. Некробиоз – необратимые дистрофические изменения
3. Гибель клетки
4. Аутолиз – разложение погибших клеток
Диагностика
· Компьютерная томография
· Магнитно-резонансная томография
· Радиоизотопное сканирование
Термин «инфаркт» известен всем нам, но мы, в основном, относим его к заболеваниям сердца, имея в виду инфаркт миокарда. В действительности инфаркт способен развиваться и в некоторых других органах, например, селезенке, легком, кишечнике, головном мозге. От локализации этого процесса зависит клиническая картина заболевания, но во всех случаях процесс этот очень серьезный.
Инфаркт — сосудистый некроз
Инфарктом в медицине зовется процесс омертвления или некроза определенного участка ткани вследствие прекращения в нем кровообращения. Самая частая причина инфарктов — закупорка сосуда тромбом, продолжительный спазм, эмболия, напряженная работа органа при недостаточном притоке крови.
Синонимами являются: омертвление, сосудистый некроз, гибель клеток, ишемический некроз, «местная смерть».
Инфаркт может развиться в любых метаболически активных органах, но чаще всего этот процесс происходит в сердце, головном мозге. Встречаются и очень редкие локализации: кости и мышцы, сетчатка, печень.
Инфаркты бывают разных форм и размеров. Данные характеристики зависят от анатомии органа, в котором развился этот процесс и от состояния здоровья в целом. Инфаркты, которые имеют малые размеры и определяются только при микроскопическом исследовании, называются микроинфарктами. Как правило, они имеют благоприятный прогноз и проходят без существенного вреда для здоровья. Нередко инфаркты занимают обширные площади, например, при трансмуральном инфаркте миокарда, когда некроз охватывает все слои сердца.
В зависимости от того, в каком органе развивается ишемический некроз, инфаркты имеют свои особенности. Рассмотрим этот процесс глазами патологоанатома, заглянув внутрь организма.
Где чаще всего развивается инфаркт?

Самая частая локализация ишемического некроза — сердечная мышца. Причиной инфарктов в этом органе в основном выступают заболевания, связанные с повреждением сосудистых стенок. К таким относят атеросклероз, ревматизм, гипертоническую болезнь. Это очень распространенные патологии в нашей стране среди людей среднего возраста, исходом которых нередко бывает инфаркт.
Инфаркт миокарда не имеет определенной формы, характерным признаком является наличие красноватого венчика по периферии светлого некротизированного участка, такой вид инфаркта патологоанатомы называют белым с геморрагическим венчиком.
Инфаркты белые и красные
Инфаркт миокарда — самая частая причина смертности людей среднего и пожилого возраста. Заболевание возникает остро с сильных болей в области сердца, сопровождается чувством страха, одышкой, липким холодным потом. Если вовремя не оказать помощь, высока вероятность летального исхода.
На втором месте по частоте летальных исходов среди сосудистых заболеваний стоит инфаркт головного мозга (ишемический инсульт). Начинается заболевание также остро, характерны общие и неврологические симптомы. Из общих симптомов чаще всего наблюдается головная боль, повышение артериального давления, может отмечаться кратковременная потеря сознания. Неврологические симптомы зависят от локализации процесса.
В головном мозге развиваются белые инфаркты. Это участки размягчения мозга, которые протекают с нарушением проводящих функций, что клинически проявляется параличами. В случае возникновения инфаркта на фоне венозного застоя, но участок размягчения пропитывается кровью, в таком случае говорят о красном размягчении ткани мозга.
Инфаркты головного мозга также развиваются на фоне сосудистых заболеваний, среди которых превалируют атеросклероз и гипертоническая болезнь.
Инфаркты других органов

В легких встречается в основном геморрагический инфаркт и очень редко — белый. Ввиду особенностей кровообращения, участок некроза в ткани легкого имеет треугольную форму: основание треугольника обращено к плевре, вершина — к корню легкого. Инфаркты легкого образуются при заболеваниях, протекающих с венозным застоем. По периферии омертвевшего участка очень часто развивается воспалительная реакция.
Белый инфаркт в легочной ткани выявляют в участках склерозированной ткани.
В почках и селезенке инфаркт тоже имеет треугольную форму. В этих органах он также наиболее часто возникает при тромбозах питающих сосудов. Инфаркт почки относится к белым с геморрагическим венчиком, клинически он проявляется острой почечной недостаточностью. В селезенке развивается белый инфаркт.
Инфаркты в кишечнике — нечастое явление, но очень опасное. Размягчение стенки кишки сопровождается присоединением микробного воспаления, что быстро приводит к развитию перитонита.
Последствия инфарктов
Инфаркт — это серьезный патологический процесс, который имеет огромное значение для здоровья и жизни человека. Исход процесса зависит от размеров инфаркта, наличия сопутствующих заболеваний, реактивности организма.
Небольшие по размеру участки инфаркта могут полностью регенерироваться, не оставляя за собой серьезных изменений. Благоприятным исходом считается и рубцевание некротизированного участка. Однако не всегда это хорошо отражается на здоровье. Так, инфаркты миокарда, в последующем замещенные рубцовой тканью, в дальнейшем проявляются развитием кардиосклероза, нарушениями ритма, сердечной недостаточности.
Еще один исход ишемического некроза — инкапсулирование. Часто образование капсулы вокруг участка инфаркта развивается в головном мозге. В тканях мозга выявляют кисту на месте предшествовавшего размягчения. Этот процесс можно отнести к благоприятным исходам, так как инкапсулирование — это отграничение патологически измененных тканей от здоровых.
Неблагоприятный исход инфарктов заключается в высоком проценте летальных исходов. Инфаркт головного мозга и инфаркт миокарда в этом отношении занимают лидирующие позиции. Смертность от этих заболеваний на сегодняшний день очень высока. Если процесс захватывает большие площади, то смерть наступает в короткие сроки, и не всегда врач успевает прийти на помощь.
После перенесенных инфарктов большое количество людей становятся инвалидами, ведь поврежденный участок не восстанавливается в полной мере, нарушая полноценную работу органов.
Своевременная диагностика и проведение адекватной терапии позволяют предупредить осложнения инфарктов, но полное восстановление функций, увы, возможно в немногочисленных случаях.
Кардиология. Национальное руководства / под ред. Е. В. Шляхто – 2015
Миокардиодистрофия у детей с точки зрения патологоанатома / Глуховец Б.И. // Вопросы современной педиатрии – 2011 – Т. 10 №1
Показатели региональной сократительной способности миокарда у больных, перенесших Q-ИНФАРКТ миокарда / Хайрутдинова Г.И., Бабушкина Г.В., Буженица С.И., Булатова О.И. // Аллергология и иммунология – 2012 – Т. 13 №1
Опубликовано в 20:41 •
Рубрика: Статьи
В зависимости от типа некроза назначают определенный вид лечения. Некроз коагуляционного или сухого типа образуется в определенной элемент тела или в органе, при этом, не распространяясь на другие части организма. При сухом некрозе ткани омертвевшего типа медленно подсушиваются. Таким образом, возникает демаркационная линия, которая отделяет здоровые ткани от инфицированных.
Встречаются случаи, когда некротизированная ткань уменьшается в размере. Такой процесс получил название мумификация.
Симптомы
Основная симптоматика следующая:
- возникновение болей в области поражения, связанных с уменьшением кровоснабжения на данном участке (ишемия);
- бледный цвет кожи (вскоре мраморный);
- зона поражения становиться холодной;
- пульс выходит из нормы;
- отсутствует чувствительность;
- онемение.
При этом наблюдается длительная боль в области конечностей. В большинстве случаев наступает спазм в коллатеральных артериальных путях.
Путь распространения некроза начинается с периферической нервной системы в области конечностей, и заканчивается уровнем закупорки сосуда.
В первую очередь необходимо предпринять меры по предотвращению возникновения инфекций в зоне поражения. Для этого используются специальные жидкости, которые вводятся внутрь. Таким образом, снижается риск инфицирования.
Зачастую такой тип некроза не вызывает летальный исход или серьезные последствия для организма, так как при поражении погибают небольшие объемы тканей.
Развитие происходит у людей, иммунитет которых наиболее устойчив. Ткани, имеющие большие объемы белков и минимум жидкости, больше подвержены возникновению. Некроз проходит без патогенных микроорганизмов и не имеет отношение к заболеваниям другого вида.
Причина появления заболевания связана с неправильным кровообращением в определенной тканевой зоне. Как следствие, некроз из-за недостаточного кровообращения и минимальном объёме кислорода в организме может повлиять на поражение других органов, в число которых входят почки, надпочечники, селезенка и сердечная мышца (миокард).
В зависимости от заболевания некроз затрагивает разные части организма:
- атеросклероз и артериальный тромбоз – конечности;
- ожоги и обморожение, болезнь Рейно – ткани в области пальцев;
- тиф сыпного вида – кожные покровы.
Некроз появляется в результате проблем с кровообращением в определенной зоне. При туберкулезе и болезни сапе прогрессирует подтип коагуляционного некроза — казеозный.
При сухом некрозе безжизненные клетки не сразу теряют свой внешний вид, они могу сохранять форму в течение нескольких дней. В тоже время ядро исчезает сразу.
Рассматривая такие клетки под микроскопом можно увидеть только розовую желеобразную массу цитоплазмы. Цитоплазматические белки, за счет своего свертывания, получают определенную стойкость к действию ферментов лизосомального типа.
Такой вид некроза получил такое название за счет сухости и плотности омертвевших участков, за счет обезвоживания.
Разновидности сухого некроза
В медицине известно несколько разновидностей сухого некроза:
- ишемический – наиболее распространённый;
- ценкеровский – возникающий зачастую в области бедра и мышц передней брюшной стенки;
- казеозный – появляющийся при туберкулёзе, сифилисе лимфогрануломатозе;
- фибриноидный – происходящий в тканях соединительного типа.
Лечение сухого некроза
Остановить разрушение клеток в тканях можно двумя способами:
- хирургическое вмешательство;
- применить лечение местного типа.
Местное лечение, наиболее щадящее, и заключается в применение следующих мер: обработка области вокруг пораженного участка антисептиком; наложение повязки, пропитанной этиловым спиртом или другим обеззараживающим средством (борная кислота, хлоргексидин) и т.д. Но не всегда удается обойтись без вмешательства хирургов, так как некроз достаточно сложное заболевание.
Терапия консервативного вида сможет наладить кровообращение в зоне поражения (интимотромбэктомия, шунтирование)
Самостоятельн6о лечить данное заболевание не рекомендуется. Лучше всего обратиться к специалисту, который назначит лечение.
Процесс остановки омертвления клеток ткани достаточно сложный. Чтобы добиться восстановления организма необходимо применять радикальные меры. В таких случаях работа проводиться несколькими врачами, специализирующихся в разных областях медицины
Результаты лечения могут зависеть от нескольких факторов, включая от места подвергшегося поражению, размера участка с некрозом и от общего состояния пациента.
Разрушение тканей может оказать токсический эффект на организм больного, за счет возникновение микробов в зоне поражения. Именно поэтому первые действия направлены на обеззараживание этого участка.
Специалисты рекомендуют как можно чаще посещать докторов с целью проверки состояния своего организма. Такие процедуры смогут помочь выявить заболевание на первичной стадии, что заметно облегчит дальнейшее лечение.